Nasal and Sinus Anatomy and Function
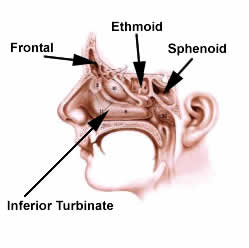 The nasal passage allows air to flow into one’s throat and lungs while being warmed, cleaned and humidified. This passage is divided into two sides by thenasal septum which when off centered (a “deviated septum”), may block air flow and cause sinus problems. The turbinates are the structures on the outer walls of the nasal passage that swell and shrink to regulate airflow through the nose. Normally one side is more swollen and the other side shrunken to allow the swollen side to re-humidify itself while air flows through the shrunken side. About every two hours the swelling switches to the other side. This “nasal cycle” is usually not noticeable unless one breathes deeply through the nose. The turbinates become more swollen when one lies down because the heart doesn’t have to pump blood uphill to them like it does when we are standing. When lying on one’s side, the turbinate on the down side becomes more swollen. Colds and allergies also cause the turbinates to be swollen or congested.
The nasal passage allows air to flow into one’s throat and lungs while being warmed, cleaned and humidified. This passage is divided into two sides by thenasal septum which when off centered (a “deviated septum”), may block air flow and cause sinus problems. The turbinates are the structures on the outer walls of the nasal passage that swell and shrink to regulate airflow through the nose. Normally one side is more swollen and the other side shrunken to allow the swollen side to re-humidify itself while air flows through the shrunken side. About every two hours the swelling switches to the other side. This “nasal cycle” is usually not noticeable unless one breathes deeply through the nose. The turbinates become more swollen when one lies down because the heart doesn’t have to pump blood uphill to them like it does when we are standing. When lying on one’s side, the turbinate on the down side becomes more swollen. Colds and allergies also cause the turbinates to be swollen or congested.
Sinuses are air pockets in the facial bones surrounding the nose, which drain into the nasal passage. They deliver clean mucous into the nose to help humidify the air and trap dust and dirt. The sinuses also make our head lighter than it would be if it was solid bone, and protect our eyes and brain by absorbing energy as they fracture. There are four sinuses on each side of the nose-frontal, ethmoid, maxillary, and sphenoid sinuses. The sinuses drain into the nose through the space between the inferior and middle turbinate.
The sense of smell occurs in the top of the nasal passage where special cells called olfactory cells are stimulated by the chemical particles that cause odors. These cells once stimulated send nerve messages to the brain. If nasal conditions keep the odors from reaching the smell cells or if viruses attack these cells the sense of smell may be 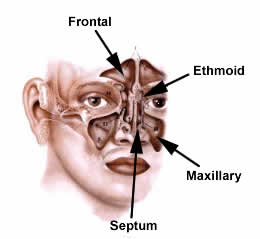 temporarily or permanently lost. Rarely, conditions of the brain can cause loss of smell. Interestingly, 75% of what things taste like, (flavor), is what they smell like. Thus if smell is lost flavor suffers greatly. In this situation one still retains the function of the taste buds, and can distinguish the four tastes: sweet, sour, bitter and salt.
temporarily or permanently lost. Rarely, conditions of the brain can cause loss of smell. Interestingly, 75% of what things taste like, (flavor), is what they smell like. Thus if smell is lost flavor suffers greatly. In this situation one still retains the function of the taste buds, and can distinguish the four tastes: sweet, sour, bitter and salt.
Sinus and Nasal Disease
Blockage of the nasal passage or nasal obstruction can be caused by a variety of conditions. A deviated septum is quite common and only requires surgical correction if it causes bothersome nasal obstruction on an ongoing basis or is contributing to sinus disease. Sometimes it is also necessary to reduce the size of the turbinates either surgically or through radio frequency reduction. Allergies are typically treated by avoiding the offending source if possible, as well as the use of medications such as antihistamines, decongestants pills, or nasal steroid sprays. Allergy shots can also be useful in patients with more severe problems or in whom medications fail. Over the counter decongestant nasal sprays should be used only for a few days, as the nose rapidly becomes dependent on them. Saline (salt water) nasal spray may be used regularly. Enlarged adenoids can also cause nasal obstruction. This is a common cause in children, but rarely occurs in adults as the adenoids usually shrink away in the teen years.
Nasal polyps typically cause nasal obstruction, but also may cause loss of smell and sinus disease. Polyps on both sides of the nose are usually an overgrowth of the lining tissue of the nose in response to allergic irritation. It appears that there is a genetic tendency to form polyps. Patients with polyps often have asthma and may be allergic to aspirin. Polyps can be difficult to manage and often require the ongoing use of steroid nasal spray, occasional doses of steroids by mouth or injection, and at times, surgery. Polyps on just one side of the nose are usually due to inflammation or infection but occasionally may be a tumor or cancer. These types of polyps usually need to be surgically removed or at least biopsied. If you think you may have nasal polyps it is important to see an ear, nose and throat specialist fairly soon.
Sinusitis (sinus infection) occurs typically when the drainage pathway of one or more of the sinuses becomes blocked. This blockage can either be due swelling of the nasal and sinus lining due a cold or allergy, polyps, a deviated septum, or changes in how the nasal structures are shaped. Often it is a combination of these factors that leads to a sinus infection. This blockage allows bacteria to move into the sinus from the nasal passage where it multiplies in the stagnant mucous. Occasionally anabnormality of the immune system may also cause sinusitis.
Although a sinus infection can be diagnosed with certainty only by x-ray or with the telescopic observation of pus draining into the nose from the sinus, a presumptive diagnosis is often made from symptoms typically seen with sinusitis. These symptoms may include colored nasal drainage from the front of the nose, fever, pain or pressure directly over the sinuses, foul breath, colored mucous in the throat, cough, and nasal blockage. Symptoms of a chronic sinus infection are similar but usually milder. It is important not to mistake a cold, which can have many of the same symptoms, for a sinus infection. Colds usually have body aches, less in the way of colored drainage, and resolve by themselves in 7 to 10 days. It is usually not recommended to seek care or treatment for a “sinus infection” unless one has colored drainage for over 7 to 10 days. The improper use of antibiotics is costly and may lead to antibiotic resistant infections down the line.
Typical treatment for acute sinusitis (lasting a few weeks) includes an antibiotic, often a decongestant pill, and perhaps the limited use (three days maximum) of a decongestant nasal spray. If after a few courses of antibiotics the symptoms fail to improve then some x-rays and/or and evaluation by an ear, nose and throat specialist should be considered. Rarely it may be necessary to rinse the infected sinus out in the office. Rarely surgery is needed. Occasionally a sinus infection will extend out of the sinus to involve the eye socket, facial skin, or other structures. This usually requires hospitalization, IV antibiotics, and often times urgent surgery.
Treatment for chronic sinusitis (lasting weeks to months) or recurring sinusitis (4 or more episodes a year) requires accurate diagnosis followed by a careful assessment of factors causing the sinusitis which typically includes a thorough discussion of the patient’s symptoms, an endoscopic (or telescopic) office examination of the nose, usually a CAT scan and, at times, allergy testing. A treatment plan of these causative factors is then developed. When medical therapy fails, or if it is clear that structural abnormalities are a major factor, then surgery may be considered.
Sinus or Nasal Surgery
Sinus or Nasal surgery is considered if other measures have failed or seem unlikely to help. This decision is reached after a discussion of the discomforts and risks involved as well as the likelihood that the surgery would resolve or significantly improve the problem.
Specifically which sinus or nasal operations are to be done can only be determined by a thorough consultation with your Ear, Nose and Throat Center physician. What might be involved in any particular case will vary, but some general guidelines are given below.
Before Surgery
- Do not take any aspirin, Motrin, Advil, nuprin, ibuprofen, Aleve, naprosyn, Peptobismal, garlic pills, ginko, and vitamin E or similar products for two weeks before surgery as these medications can promote bleeding. Avoid these medications and products for two weeks after surgery also. You may take tylenol.
- Please be sure to get any preoperative blood work or tests done in a timely fashion.
- DO NOT EAT OR DRINK ANYTHING AFTER MIDNIGHT (not even water) the day before surgery. Otherwise it may be necessary to cancel surgery.
- If you have any questions about your surgery please call the office in a timely fashion.
The Day of Surgery
- DO NOT EAT OR DRINK ANYTHING THE MORNING OF SURGERY.
- If you take any medications regularly please be sure to ask which ones you should take (with a minimal sip of water) the morning of surgery.
- You will need to arrive at the surgical facility well before the scheduled time of surgery. A day or two before surgery you will be called by the doctor’s nurse or someone from the facility with specifically what time to arrive.
After Surgery
- Depending on what is being done, your operation will last one to four hours. A family member should remain in the waiting room until the doctor speaks with them after surgery.
- You will usually go home one to four hours after surgery, depending on the time and extent of your surgery. You should plan to have someone drive you home after surgery as you will be unable to drive.
- Keep your head elevated as much as possible after surgery. You may sleep flat.
- You will usually have packing in both or just one side of your nose. This will be removed in the office two to five days after surgery. Someone should drive you to and from this first appointment. After the packing is removed you should
- go directly home and rest quietly the rest of the day.
- avoid blowing your nose for two weeks, you should open your mouth to sneeze
- avoid strenuous activity for two weeks.
Returning to Work
Depending on the specific surgery that has been performed, your level of discomfort, and the nature of your job, you may return to work the day after the packing is out or you may need to wait for up to two weeks. Please discuss this with your Ear, Nose and Throat Center physician.
Follow-up Care
You will need to return to the office every week or two for one to two months following surgery for the nose to be cleaned and examined to insure all is healing well. Adults may drive themselves to these appointments.
Risks Of Surgery
Although the chances of complications from surgery are typically quite low, there are no “risk-free” operations. The following information is provided not to frighten patients, but rather that they might be informed. Some common nasal and sinus surgical procedures are listed below. The lay terms for these procedures and most of the possible risks of each procedure are also listed. The general risks of any surgical procedure include those related to anesthesia, infection, bleeding, and scar tissue formation. Due to allergies, scarring, or other factors, recurrence of sinus or nasal problems after surgery is always possible.
Nasal Septal Reconstruction straighten middle cartilage and bone inside nose): Possible risks* include nasal blockage, crusting, hole in nasal septum.
Partial resection of lower and/or middle turbinates (remove part of lower and/or middle nasal swell bodies): Possible risks*include nasal crusting or dryness.
Middle Meatal Antrostomy (open into cheek bone sinus): Possible risks*include closure of opening by scar tissue; blockage of, or airflow through tear duct; eye bruising, swelling, damage, or very rarely blindness.
Partial or Total Ethmoidectomy (open up honeycomb sinuses next to eye-socket): possible risks* include loss of smell; or very rarely eye bruising, swelling, damage, blindness; spinal fluid leak; meningitis.
Sphenotomy (open rear nasal sinus): Possible risks* include closure of opening by scar tissue.
Frontal Sinus Exploration or Frontal Sinusotomy (open into forehead sinus): Possible risks* include closure of opening by scar tissue; or very rarely eye bruising, swelling, damage, blindness; spinal fluid leak; meningitis
Maxillary Sinus Endoscopy with Removal of Cyst or Polyp (look into cheekbone sinus through nose and remove tissue): Possible risks* include recurrence of cyst or polyp.
Caldwell Luc (open cheekbone sinus and remove lining through incision under lip): Possible risks* include permanent numbness of lip or teeth; failure of incision into sinus to close, inability to wear present dentures.
Nasal Polypectomy (remove polyps from nose): Possible risks*include recurrence of polyps requiring further medical or surgical treatment. Some types of polyps have a strong tendency to recur.
*Possible risks include but are not limited to those listed.