Other words that patients would use for ear fullness would include plugging, congested, hollow or cotton feeling. Patients use the same words to describe significantly different clinical conditions, which if misdiagnosed, may involve incorrect treatment.
The most important condition is sudden sensorineural hearing loss (SSNHL). The etiology is not certain, but the probable theories include viral, vascular or inner ear membrane rupture. Oral steroids medications within the first seven days offer the best outcome for these patients. Thus there is a “window of opportunity” for treating this loss that is lost if accurate diagnosis is delayed. These patients present with a history of normal hearing one day followed the next day by no or very poor hearing. They deny ear pain, may note vertigo or imbalance but frequently complain about ear fullness or pressure which leads to inappropriate treatment with antihistamines/decongestant and/or antibiotics.
Another less urgent condition involves cochlear hydrops (buildup of inner ear fluid), which is a variant of endolymphatic hydrops (Ménière’s Disease), and has a gradual, nonspecific onset with fluctuating intensity. This is treated with a low salt (sodium) diet and diuretics but not with decongestants or nasal steroid sprays.
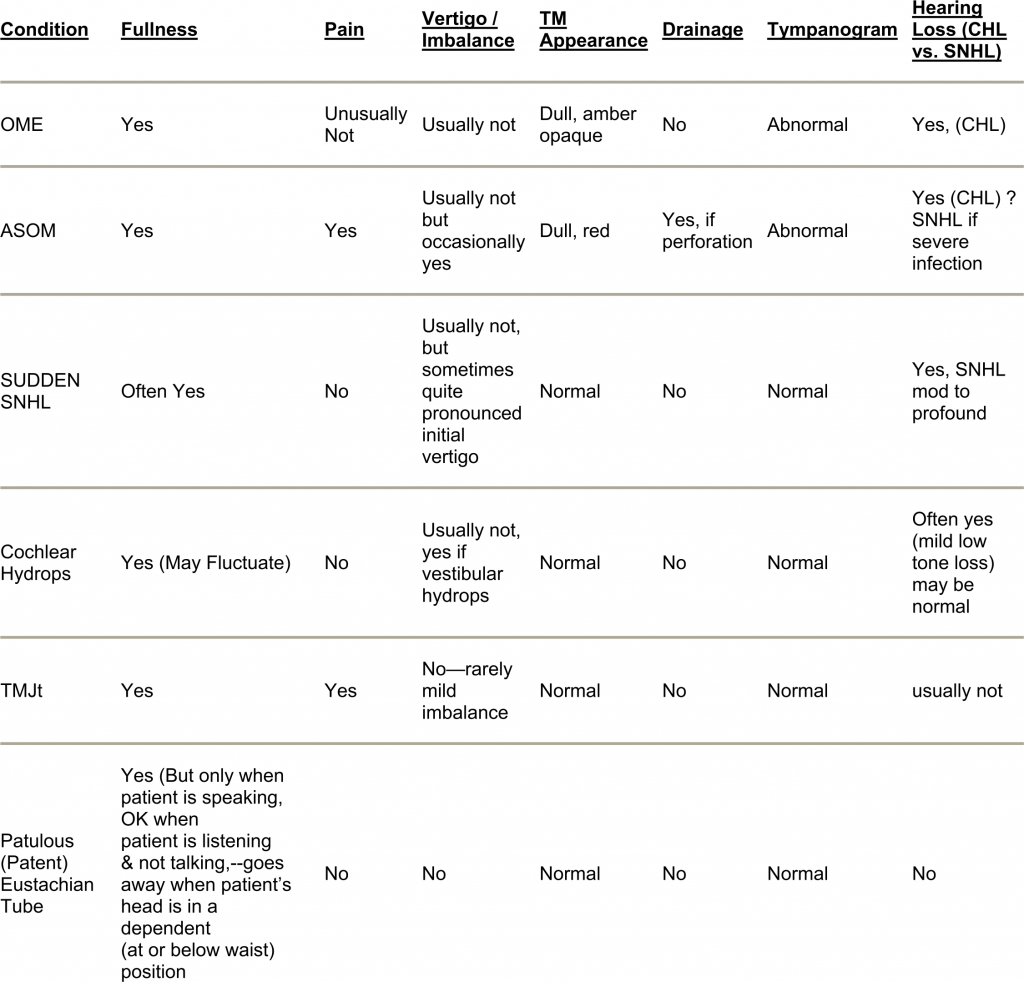
Other conditions with ear fullness symptoms include Temporal Mandibular Joint (TMJt)/myofacial abnormalities, patulous (patent) eustachian tube, otitis media with effusion (OME), and acute suppurative otitis media (ASOM). The last two conditions should have evidence of a conductive hearing loss (CHL) and an abnormal tympanogram.
The following chart shows the characteristics about these clinical entities: